While both aim to improve healthcare outcomes, care coordination is broader, emphasizing continuous, integrated care, whereas case management is more focused and structured around specific health issues.
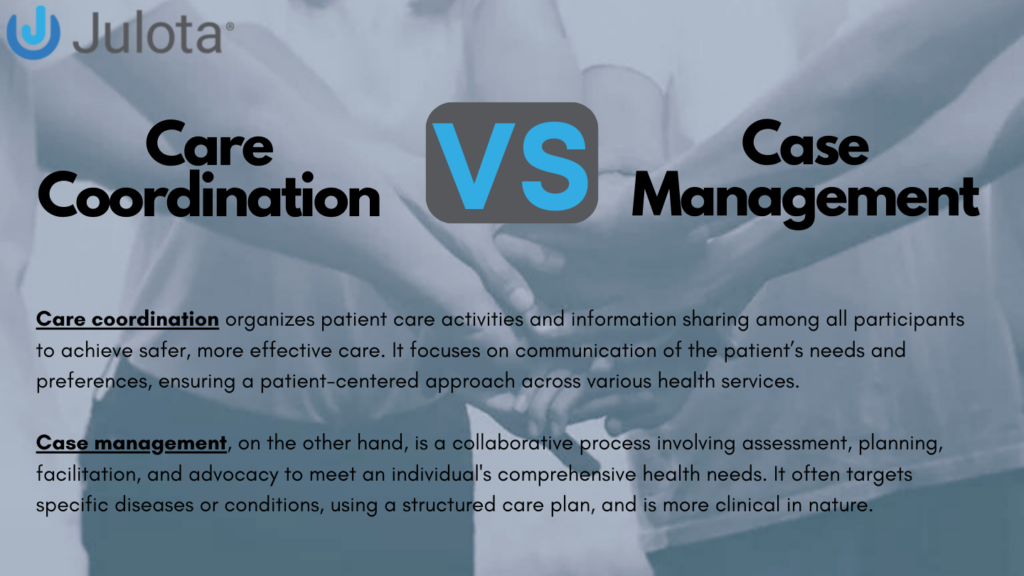
Care coordination organizes patient care activities and information sharing among all participants to achieve safer, more effective care. It focuses on communication of the patient’s needs and preferences, ensuring a patient-centered approach across various health services.
Case management, on the other hand, is a collaborative process involving assessment, planning, facilitation, and advocacy to meet an individual’s comprehensive health needs. It often targets specific diseases or conditions, using a structured care plan, and is more clinical in nature.
The Evolution of Care Coordination and Case Management
The health care system has multiple players, including employees, insurance companies, managed care companies, health service professionals, health service organizations, and the government. members perform specific tasks but collaborate to meet the patient health care needs.
Over the years, the healthcare delivery system has experienced rapid and dramatic changes from acute care to outpatient and community settings. Many factors have facilitated this change, most which aim to reduce costs, such as developing new technology.
In addition, changes have been aimed at improving healthcare quality and access, such as care coordination and case management. This is an attempt to compare the two systems to understand the role each has played in the healthcare space.
Case management and care coordination are terms that pose confusion not only among the patients but also among healthcare providers. According to the Case Management Society of America, case management ‘is a collaborative process of assessment, planning, facilitation, care coordination, evaluation and advocacy for options and services to meet an individual’s and family comprehensive health needs through communication and available resources to promote quality and cost-effective outcomes.’
It is not a new development because it dates to the 1980s when managed care was started with an emphasis on welfare, health promotion, and illness prevention. The early movements to contain health care costs led to the formation of Health Maintenance Organizations and the Preferred Provider Organizations that provided managed care using case management.
The Agency for Healthcare Research and Quality (AHRQ) describes care coordination as “deliberately organizing patient care activities and sharing information among all of the participants concerned with a patient’s care to achieve safer and more effective care.” Key among the components of care coordination is the communication of the patient’s needs and preferences.
Client-Centric Approach to Care Coordination
What stands out in the care coordination process is its client-centric approach. The coordinator’s role is to ensure that all the other participants are duly involved and informed of the client’s preferences.
There are some differences and similarities between the two. From the service provider’s point of view, in most cases, it is the same cadre of healthcare providers, called a case manager or a care coordinator, who provides the services. Most additionally hold physicians, nurses, or social worker’s licenses.
Ontologically, all case management involves an element of care coordination, but not all care coordination merits being called case management. In case management, one looks at the disease from a pathological perspective and a human perspective. With care coordination, there is a particular emphasis on linking healthcare components from various sources and supporting information sharing across providers, patients, types and levels of service, sites, and time frames.
In some population health systems, a case manager, who usually has a degree in nursing or social work, oversees the care coordinator, who may not have a Bachelor’s degree.
Single Illness Versus Patient-Centered Care
The other difference is that case management is often directed towards a single illness, while care coordination is a patient-centered, consistent care approach across multiple illnesses. Take the example of Integrated Management of Childhood Illness (IMCI), developed by the World Health Organization (WHO), the United Nations Children’s Fund (UNICEF), and other partners to reduce death, frequency, the severity of illness and disability, and to contribute to improved growth and development.
The IMCI case management process is presented in a series of charts that show all the procedures and information for performing them. It looks very efficient and empirical, but it tends to reduce healthcare into medical algorithms.
On the contrary, care coordination envisions individually tailored care for the patient, which can be very useful for those with chronic conditions, which sometimes lead them to visit different healthcare providers. Through care coordination, the care plan formulated looks at their medical conditions and considers other factors like their support system.
It is a more comprehensive approach that looks at the clinical and non-clinical components as an interwoven thread. The goal of care coordination is to help link patients and families to services that optimize outcomes articulated in a patient-centered care plan. In addition, care coordination may address patients’ and families’ social, developmental, educational, and financial needs.
It often includes activities that may or may not be covered by defined benefits.
Models of Case Management and Care Coordination
The models used to implement case management and care coordination also differentiate them. Care coordination attempts to provide a longitudinal or holistic approach, making in-person meetings almost inevitable.
On the contrary, with the advent of telehealth, case management has the option of being purely online. Of course, telehealth also presupposes an initial in-person contact, but the availability of the telehealth option during case management marks the difference.
For example, in what qualifies as a complete visit in case management, the healthcare team can call the patients after discharge from a hospital to ensure that the treatment plan is being followed by asking specific questions, addressing any early symptoms, and offering health education.
Data Collection
Case management and care coordination also differ in the type of information each generates. Case management is case-specific and is guided by a care plan ‘developed collaboratively by the patient and the care providers, which is designed and executed to optimize the patient’s health status and quality of life.‘
In care coordination, there are different participants, including the patient, and it involves marshaling personnel and other resources needed to carry out all the required patient-care activities.
The difference in the data allocated also has implications for the type of health technology that can be applied. For example, care management is primarily clinical. As a result, most models are centered in a hospital or a community health center.
The tools significantly depend on the access to clinical data to ensure that providers can make informed, proactive decisions about an individual’s acute needs. On the contrary, care coordination takes place in a myriad of settings. Therefore, it requires enhanced access to data about a patient’s social determinants of health and their clinical status.
Its holistic approach demands that the health technology communicates with other stakeholders while maintaining fundamental patient rights like privacy and confidentiality. Luckily, the push toward managed care and value-based payments has stimulated significant investment in care coordination to facilitate tech-enabled care coordination between patients, providers, and their care teams.
Care Coordination Technology
One of the most promising care coordination platforms on the market is Julota. Julota transforms the disconnected patchwork of local service providers into a well-coordinated network that can proactively manage and support individuals, saving each community millions of dollars in healthcare and operational expenditures
For several stakeholders in the health sector, the issue of costs is always elusive. Many people are always keen to see how a healthcare system alleviates the costs—concluding that case management or care coordination, owing to the complexity of processes involved, is more expensive and looks more of rustic simplicity.
This is one of the benefits that link them.
Individuals who receive case management typically require services likely to result in high costs and have complex medical needs. However, several studies have shown the cost-effectiveness of case management.
For example, a study to quantify the benefits in terms of health effects [quality-adjusted life years (QALYs)] and costs when heart failure patients receive case management at home compared with outpatient cardiology clinic follow-up showed that case management is cost-effective in 83.3% of the probabilistic simulations and has a tendency towards reducing costs and increasing QALYs.
In a study to evaluate a care coordination program to provide combined “whole-person care,” integrating medical, behavioral, and social support for high-cost, high-need Medicaid beneficiaries, the results showed that such a system resulted in fewer ED visits and hospitalizations for patients with diabetes. The study also shows varying results among different Medicare providers since some are not structured to deliver such coordinated services.
A different study that compared two other models of care coordination, the public-private collaboration model vs. traditional management, showed that the former is more efficient in chronic illness care coordination because of its collaborative nature.
The benefits of care coordination are not limited to the costs. Other benefits attributed to care coordination include ‘decreasing duplicate services, lowering the overuse of more intense procedures, decreasing preventable hospital admissions and re-admissions, improving overall patient experiences, and offering more comprehensive, interdisciplinary care.
Despite the attempt to pin the differences between case management and care coordination, there is much interdependence between the two models of care. Powerful and effective case management is essential to establishing lasting care coordination. Focusing on one element alone might not be the best solution. The demonstrated benefits undoubtedly call for improvement in the design and implementation.